No one could have imagined the impact the COVID-19 pandemic would have on society, and the tragic toll on human life. As across pathology, the cytology community has struggled with huge changes not only in our personal lives, but also in working practices.1
Cytology samples
In common with other areas of pathology, cytopathology services have experienced a significant reduction in demand during the pandemic. Nevertheless, diagnostic cytology remains central to cancer diagnosis, and laboratories are still receiving bronchoscopy specimens, pleural and peritoneal fluids/washings, and urine and cerebrospinal fluid samples. As many cytology samples are received fresh and considered potentially hazardous, cytopathology laboratories are used to handling samples in compliance with the control of infection guidance. However, all procedures have had to be revisited in the light of COVID-19 guidance.2
Many cytopathology samples are derived from fine needle aspiration (FNA). The pandemic has brought into sharp focus the need for safe handling of potentially infective (from all causes) aspirated material, particularly with respect to appropriate personal protective equipment (PPE) and a safe working environment. Although cytopathologist and radiologist performed FNA have been limited to urgent referrals, it has been important to find safe ways of continuing FNA services, given its valuable role as a triage and diagnostic tool for suspected malignant lesions, including lymph nodes, breast lumps and subcutaneous deposits. FNA of accessible metastatic sites have been used as a surrogate for biopsy of the primary site. Trans-oral FNA has been reported instead of tonsillar/palatal biopsy to help keep operating theatres free for emergency surgery. P16 and HPV-ISH on cell blocks from primary and metastatic site FNA have been used in new oropharyngeal cancers awaiting definitive treatment. Once routine work resumes, there will be a significant backlog, particularly with respect to endobronchial/endoscopic ultrasounds (EBUS/EUS), thyroid and head and neck FNA, for which cytopathologists should be prepared.
The pandemic has brought into sharp focus the need for safe handling of potentially infective (from all causes) aspirated material, particularly with respect to appropriate personal protective equipment (PPE) and a safe working environment.
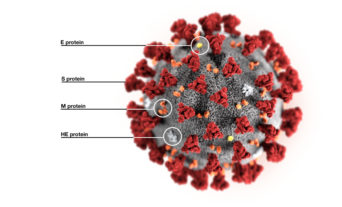
The WHO has recommended that all cytology samples are immersed in at least 70% alcohol, which has been shown to inactivate coronaviruses. As such, the ability to offer EBUS rapid onsite evaluation or immediate reporting has been compromised. Many samples nowadays are taken into a liquid preservative (liquid-based cytology). This may contain fixatives other than 70% ethanol, and most, if not all, labs have had to modify laboratory protocols3 to handle the collection and processing of samples. The previous ease of use of samples using liquid-based cytology preservatives and methodology has been made more problematic with these additional requirements.
Cervical cytology
Departments that offer cervical cytology have seen a huge reduction in demand. All four UK countries did pause non-urgent routine call/recall invitations, but this was not done uniformly. Women have experienced local variations in the availability of screening, although this was not driven by the laboratories. Professional bodies including the College produced guidance agreed by NHS England and NHS Improvement (NHS EI), but this exposed a lack of agreement and unified action between those responsible for testing and screening in England. The reduction in routine workload during the pandemic has allowed laboratories to largely clear backlogs that had developed following the introduction of the primary HPV cervical screening program.
With the rapid introduction of COVID-19 testing, cervical screening providers and commissioners were not always fully involved in decisions on prioritisation of use of platforms that can be used for both tests. The Roche Cobas platforms proved ideal for early implementation of COVID-19 testing and have in some laboratories been refocused on this. The ability to run both tests on the same platform or even within the same laboratory seems to vary between centres. Practical use of the Hologic Aptima test platforms for COVID-19 testing has been slower to implement. Problems with test capacity and reagent supply have been highlighted. At the time of writing, the NHS in England has been focused on restarting non-COVID services and recommencing cervical screening services, including restarting routine invitations. It is essential that protected capacity for HPV testing is ensured before sample taking returns to normal levels.
The reduction in routine workload during the pandemic has allowed laboratories to largely clear backlogs that had developed following the introduction of the primary HPV cervical screening program.
After such massive screening programme disruption, it seems doubtful that laboratories will meet many of the programme quality standards. Commissioners in England, and Screening Quality Assurance services, are taking a pragmatic approach. However, aspects of quality assurance, including incident reporting, remain very much as normal.
Impact on working practices
For pathology laboratory and medical staff, the impact of COVID-19 has meant reduced onsite staffing levels, more working from home, additional PPE, social distancing measures and remote multidisciplinary team meeting input, most of which has been rapidly implemented. The huge dependency on IT has become evident, and the NHS IT infrastructure has struggled at times to deliver. Many of the patterns of work introduced may continue as part of the ‘new normal’. It is also likely that there will be changes in clinical pathways and clinical ways of working. The use and delivery of cytopathology may never fully revert to pre-COVID ways and, in some aspects, this will be for the better.
Education and training
Significant changes have occurred in education and training. Conferences and meetings have ceased, and examinations suspended. It is difficult to see these returning in 2020. The immediate need to use web-based tools and material has accelerated the implementation of digital pathology.4 The first College specialist webinar was in cytopathology, held jointly with the British Association for Cytopathology, and attracted 300 participants. Others are being developed and this must be the model going forward. When actual meetings restart, we must not abandon online teaching, given its great flexibility and ease of access.
Social distancing has negatively impacted day-to-day supervision with less one-to-one double-headed microscope teaching.
The effect of COVID-19 restrictions on in-lab training has been felt acutely in the staff-heavy cellular pathology disciplines. Social distancing has negatively impacted day-to-day supervision with less one-to-one double-headed microscope teaching. Some have found innovative solutions such as extending double-headed microscopes or the use of cameras on consultant microscopes to show images via IT systems.
The COVID-19 pandemic has changed the world in a few short weeks. Much that was taken for granted prior to it will not happen again for at least a long while. However, many of the changes introduced in cytopathology, and across pathology and medicine, are positive ones, and should not be forgotten or abandoned. There is also much we can learn about the collective response to the pandemic, and what we can implement for the future.
Author(s)

Dr Paul Cross

Dr Ashish Chandra
Dr Louise Smart